New report detailing access and affordability challenges intends to help measure success of policy and funding changes
This story was originally published in Rhode Island Current, a publication partner of Ocean State Stories.
PROVIDENCE — An initial wellness exam for the state’s primary care landscape published by the Office of the Health Insurance Commissioner on Monday found fewer Rhode Islanders have a personal doctor they can turn to for non-urgent health concerns compared with a decade earlier.
The 31-page report, which relies on 2024 insurance claims data, marks the first in what Health Insurance Commissioner Cory King intends will serve as an annual checkup on the policy and funding ailments plaguing Rhode Island’s primary care system.
“The purpose is to establish a baseline understanding, so we can be able to judge whether the efforts undertaken actually improve the needle on primary care payment and access,” King said in an interview.

“Primary care is the cornerstone of a strong and effective health care system,” the report states. “For most patients, it serves as the entry point to care; they rely on trusted relationships with primary care clinicians for preventive services, chronic condition management, and referrals to specialists when needed. Timely access to high-quality primary care is crucial to the health and productivity of Rhode Islanders.”
Rhode Island is not alone. Financial strain, provider shortages and the behavioral shifts lingering after a COVID-19-induced shutdown have led to a drop in primary care visits nationwide.
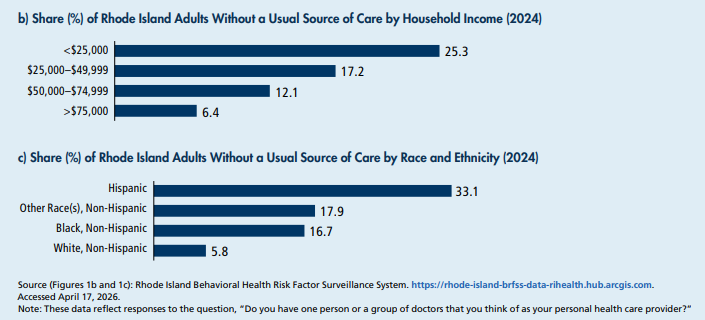
The Ocean State appears to fare better than the national average in terms of adult access overall, but demographic details reveal alarming disparities. One-third of Hispanic Rhode Islanders lack a reliable primary care doctor or nurse practitioner, more than six times the rate of their white, non-Hispanic peers. Low-income households, those that earned less than $25,000 in 2024, were more than four times as likely to report no primary care provider than households that earned $75,000 or more.
People on Medicaid are also at a disadvantage relative to their peers with commercial insurance; less than half of Rhode Islanders with Medicaid through managed care organizations had a regular wellness visit with a primary care provider in 2024, compared with nearly seven in 10 people with commercial insurance plans.
And across insurance models, people are increasingly turning to urgent care in lieu of traditional office visits with doctors, nurse practitioners and physician assistants due largely to an ever-deepening provider shortage.
Research from Brown University’s Warren Alpert Medical School referenced in OHIC’s report estimates Rhode Island needs at least 300 more primary care providers, with the 700 full-time providers unable to care for the population even at a staggering 1,700 patients per provider. Workforce burnout, retirement and moves to other states that offer competitive reimbursement rates are expected to worsen the existing provider shortage.
It’s a grim prognosis, and one that many fear will worsen under federal policy changes in the One Big Beautiful Bill Act.
New restrictions on Medicaid eligibility are expected to create a rise in uncompensated care, adding more demand and pressure to cash-poor healthcare facilities. Caps on student loan amounts will make it hard for aspiring doctors and nurses to afford advanced degrees, limiting the pipeline of providers badly needed to fill in the gaps in Rhode Island. And new limits on federal pass-through funding to states will make it even less financially feasible for providers to participate in treating patients with government or even traditional, commercial insurance — leading to a rise in private-pay “concierge medicine,” in which a limited number of patients pay a fee directly to their doctor for access.
“There’s no business reason why any primary care physician shouldn’t do direct primary care,” said Dr. Michael Fine, former state health director and president of advocacy group Primary Care for All Americans.
Referring to the rise in concierge medicine, Fine said, “What I am hearing on the street with this is, it’s turning into a tsunami.”
In search of solutions
But, there are remedies — some already in place and others under consideration — that could help heal the state’s primary care system.
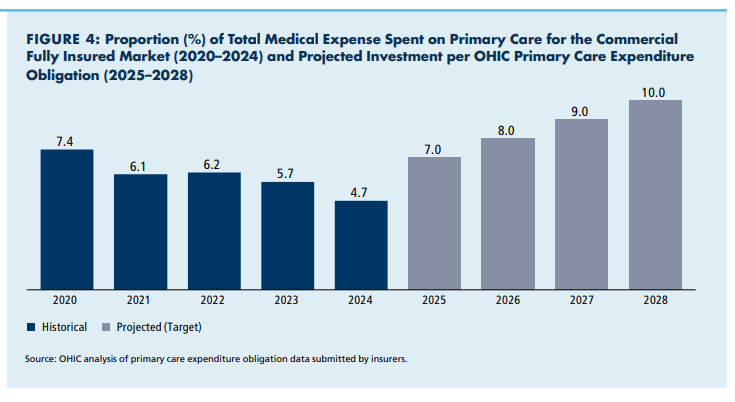
In March 2025, King’s office issued new regulations to commercial insurers, requiring them to increase their share of overall annual spending on primary care from the 4.7% spent in 2024, to 10% by 2028, while mandating they reduce prior authorization policies for providers by at least 20%. The spending mandate is expected to increase funding by $40 million over four years.
Meanwhile, a highly anticipated review of state reimbursement rates for primary care providers, measuring costs and competitiveness with neighboring states, will be issued in September.
Many expect OHIC’s forthcoming rate review will mandate further rate hikes for primary care providers, who receive 30% less than their Massachusetts counterparts for the same services, on average, from commercial payers, according to the OHIC report. Medicaid and Medicare reimbursement comparisons are less stark, but still favor Massachusetts providers.
Commercial insurers have historically pushed back on the rate differences between Rhode Island and Massachusetts, citing the cost-of-living differences. King acknowledged that it’s unreasonable to expect the Ocean State to match its northern neighbor on all types of medical service payments. But given the importance of primary care, a matching rate might be needed, he said.
Meanwhile, lawmakers are finalizing a fiscal 2027 spending plan that, at last revision, is set to include a $5 million seed fund for a medical school at the University of Rhode Island. The long-awaited creation of a state medical school is one of several measures intended to attract and retain new primary care providers, along with enhanced student loan forgiveness (also bolstered in the revised House fiscal 2027 budget) and scholarships.
The Senate Committee on Finance is scheduled to advance a bill Tuesday that would set up a scholarship fund for doctors, nurse practitioners and physician assistants who stay and work in Rhode Island for twice the number of years they receive educational scholarship funds. The $1 million price tag was not included in the revised fiscal 2027 budget, but Sen. Pam Lauria, the bill’s sponsor, remains optimistic.
“I know the budget is being discussed in both chambers, and this is something the Senate is committed to,” Lauria, a Barrington Democrat and nurse practitioner, said in an interview.
A House companion bill by Rep. Kathleen Fogarty, a South Kingstown Democrat, remains under review in the chamber’s finance committee following an April 30 hearing.
Asked for comment on the scholarship bill, Larry Berman, a spokesperson for House Speaker Christopher Blazejewski, said the revised fiscal 2027 budget added more money for loan forgiveness plans for primary care providers, including through the state’s Wavemaker fellowship program.
A spokesperson Senate President Valarie Lawson did not immediately respond to requests for comment Monday.
Tackling self-insured employers
King is also considering how to leverage his office’s authority over self-insured employers, responsible for coverage for roughly two-thirds of Rhode Islanders.
Unlike businesses that transfer all the risk of health coverage for their workers to third-party insurers, or self-insured individuals, King’s office has no power to set annual premium rates for these private companies, including top employers like the state of Rhode Island and many of the major hospital and healthcare groups.
Blue Cross Blue Shield of Rhode Island voluntarily raised its primary care provider rates for its self-insured employee plan last year, with the intent of investing more than $50 million through 2028.
“These investments will improve financial stability for practices, support recruitment and retention, and help expand access to care at a time when primary care continues to face workforce and financial pressures,” Rich Salit, a company spokesperson, said in an email.
Goodwill might not be enough to spur other self-insured employers to follow suit. So King is contemplating mandates by way of the insurance companies that act as third-party administrators to business-funded plans.
“If we’re really committed to primary care, it’s worth exploring whether we can or should require self-insured employers to invest in primary care,” he said.
Lauria backed the proposal, noting that her own employer, Brown University Health, has not voluntarily agreed to increase its reimbursement rates to primary care providers.
Brown University Health did not immediately respond to requests for comment Monday.
Fine remained skeptical that any of the small measures taken or under consideration were enough to save a broken healthcare system.
“I don’t care about where the deck chairs are on the Titanic,” he said. “What I care about is that we are sailing the Queen Elizabeth and not the Titanic.”
His proposal? A “Marshall Plan,” that includes strategic and coordinated oversight of providers, and private and public insurance payors, while also addressing geographic distribution of primary care offices and the demographic barriers to care.
Fine’s advocacy group, Primary Care for All Americans, recently held its inaugural summit in Cambridge, Massachusetts, featuring top research and healthcare leaders discussing various models for improving primary care, including a universal care model.
“Cory did a great thing by throwing down this gauntlet,” Fine said of the report. “But his authority only extends so far.”